Dr Matelic and Dr Shawn Brandenburg publish article on a Complication of ACL Reconstruction and how to correct it
Loss of Internal Tibial Rotation After Anterior Cruciate Ligament Reconstruction.
Abstract
The flexion angle of the knee and the position of the tibia need to be considered during tensioning of the anterior cruciate ligament (ACL) graft to avoid overconstraining the knee. The purpose of this report was to describe 2 cases of loss of tibial internal rotation after single-bundle anatomic ACL reconstruction with graft tensioning in flexion. Retrospective review of each patient’s operative chart revealed that the graft was tensioned in flexion and placed in an anatomic position in the femoral tunnel at the time of the index operation. Primary outcome was ACL revision surgery. Secondary outcome data included Lysholm scores and Lachman and pivot shift tests. Two patients underwent revision ACL reconstruction with a more vertical tunnel placed through a transtibial technique. The graft was tensioned in full knee extension and neutral rotation of the tibia. This resulted in restoration of normal tibial internal rotation to 10°. Lysholm scores improved from 35 to 90 in patient 1 and from 12 to 61 in patient 2. Patient 1 returned to college soccer at 6 months postoperatively. Her knee was stable to Lachman and pivot shift tests. Patient 2 has been followed for 12 months and has returned to all normal activities without pain or dysfunction. Anatomic femoral placement of the ACL with improper positioning of the knee during tensioning of the graft may capture the knee and lead to loss of the normal internal rotation. The surgeon should be aware of this complication during primary ACL reconstruction. [Orthopedics. 2018; 41(1):e22-e26.].
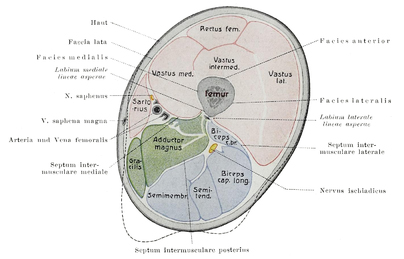 During Game 4 of the Nashville Predators game with the Anaheim Ducks Ryan Johansen suffered an injury to his left thigh. Most likely he sustained a significant contusion to his thigh during a collision with another player or the wall. While at first, he may have been sore and maybe even continued to play, the contusion resulted in tearing of a muscle and as the muscle bleeds like most tissue in our body, the bleeding resulted in a hematoma. A hematoma is just a collection of blood like you would see under a bad blister. However, in this case the bleeding was more severe and the collection of blood became quite large. In the extremities, this can be dangerous because muscles are in compartments surrounded by a thin but tough layer of fibrous tissue called fascia. Think of this like a skin around a link of sausage. When the bleeding becomes too intense the muscle within the tight compartment swells (like when a sausage link cooks in a pan). The pressure inside this compartment becomes so great that the normal blood flow and oxygen that the blood carries to the cells cannot get into the muscle. It is like putting a tourniquet around the muscles of his thigh. This is called an acute compartment syndrome. It is more common in major traumatic injuries and often associated with fractures. If this condition goes on for too long, the muscle actually dies. This would obviously have long term consequences for the athlete. In the surgery, an incision is made over the compartment of the thigh where the pressure is too high due to the bleeding. The skin and fascia surrounding the muscle is opened and the hematoma is removed. This releases the pressure and restores the normal blood flow to the muscle, and the muscle is allowed to ” breathe” again. The skin is usually left open until the swelling resolves and the hematoma stops forming and then it is closed usually within a few days. When this injury is found early as it was in this case and treated appropriately it will result in no long term complications. The athlete will be able to return to sport without difficulty usually within two to three months. If it is missed and not treated it could result in permanent damage and loss of muscle or limb function or even amputation.
During Game 4 of the Nashville Predators game with the Anaheim Ducks Ryan Johansen suffered an injury to his left thigh. Most likely he sustained a significant contusion to his thigh during a collision with another player or the wall. While at first, he may have been sore and maybe even continued to play, the contusion resulted in tearing of a muscle and as the muscle bleeds like most tissue in our body, the bleeding resulted in a hematoma. A hematoma is just a collection of blood like you would see under a bad blister. However, in this case the bleeding was more severe and the collection of blood became quite large. In the extremities, this can be dangerous because muscles are in compartments surrounded by a thin but tough layer of fibrous tissue called fascia. Think of this like a skin around a link of sausage. When the bleeding becomes too intense the muscle within the tight compartment swells (like when a sausage link cooks in a pan). The pressure inside this compartment becomes so great that the normal blood flow and oxygen that the blood carries to the cells cannot get into the muscle. It is like putting a tourniquet around the muscles of his thigh. This is called an acute compartment syndrome. It is more common in major traumatic injuries and often associated with fractures. If this condition goes on for too long, the muscle actually dies. This would obviously have long term consequences for the athlete. In the surgery, an incision is made over the compartment of the thigh where the pressure is too high due to the bleeding. The skin and fascia surrounding the muscle is opened and the hematoma is removed. This releases the pressure and restores the normal blood flow to the muscle, and the muscle is allowed to ” breathe” again. The skin is usually left open until the swelling resolves and the hematoma stops forming and then it is closed usually within a few days. When this injury is found early as it was in this case and treated appropriately it will result in no long term complications. The athlete will be able to return to sport without difficulty usually within two to three months. If it is missed and not treated it could result in permanent damage and loss of muscle or limb function or even amputation.